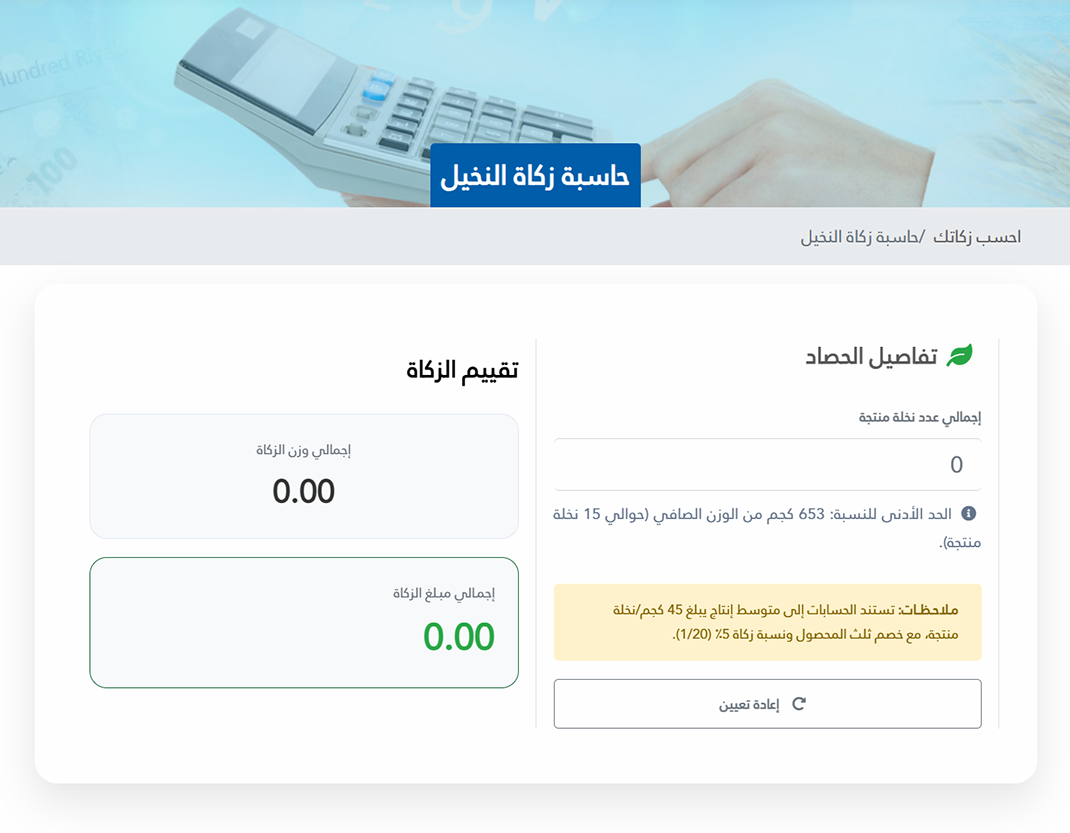
حساب زكاة النخيل
تكشف تجربة زكاة النخيل في قطر كيف يمكن للاجتهاد الفقهي أن يواكب الواقع عبر التكامل بين الأحكام الشرعية والخبرة الزراعية والتقنيات الحديثة، فمن خلال حاسبة إلكترونية مبنية على أسس علمية وفقهية، أصبح أداء الزكاة أكثر يسراً دون إخلال بالجانب الشرعي المرتبط بها.